








The Center for Kidney Stones Disease at MedStar Health has more than 30 years of experience treating the most complicated kidney stone patients in the metropolitan area. We offer patients prompt evaluation and effective treatment options, including medical support to help patients pass stones spontaneously when possible.
We also provide the most advanced technology to help remove stones when surgical treatment is necessary. When the acute event is resolved, we offer effective medical evaluation to help patients define the causes of their stone formation to help prevent stone recurrences.
New technologies help doctors manage kidney stones. Imaging studies help doctors diagnose stones quickly and reliably, before kidney damage happens. Modern surgery for stones is effective, minimally invasive, and often performed as an outpatient procedure. Medications and diet advice can prevent stones from growing or returning. Better diagnosis, treatments, and prevention mean quick recovery and fewer repeat episodes.
Kidney stones, solid deposits of mineral and acid salts that build up inside the kidneys, are relatively common – more than one million Americans are hospitalized every year with this condition, and approximately 10 percent of people in the United States will have a kidney stone sometime in their life.
Kidney Stones

Occasionally calculi,or crystals, form in a kidney and are referred to as kidney stones.
Risk factors for kidney stones include
-
Whites are more likely to develop kidney stones than African Americans or other races.
-
Men are more likely than women to have stones, but the number of women with stones has gone up in the past ten years.
-
This may be connected to the rise in obesity in women compared to men, as obesity is a known risk factor for kidney stones.
Types of kidney stones
-
The most common stone composition is calcium oxalate. These stone can also have a small percentage of calcium phosphate.
-
Patients with recurrent urinary tract infections may have stones made of magnesium ammonium phosphate (struvite). The bacteria in the urine cause the urine pH to become basic and this causes the stone salts to precipitate out rapidly and these stones can become large and fill the kidney (they may look like a dear antler).
-
Less common stone composition includes uric acid stones in about 8 to 10 percent of patients and even less common are stones composed of cystine. This is an amino acid one of the building blocks of proteins and they tend to develop in children around the onset of puberty.
Symptoms of kidney stones
If a urinary stone is in the kidney and not blocking the passage of urine it may not cause symptoms. Blood may be found in the urine during a routine urine exam (urinalysis) and may suggest the presence of a urinary stone. Stones that are associated with urinary tract infection may be found when looking for causes of persistent UTI. Most stones that pass out of the kidney are 4 mm in size (about the size of the head of a match). This size stone causes blockage of urine flow when it enters the ureter and causes a rapid swelling (hydronephrosis) of the kidney. Symptoms may include:
-
Sharp, cramping pain in the back and side, often moving to the lower abdomen or groin. Some say the pain is worse than childbirth labor pains. The pain often begins suddenly and comes in waves. It can come and go as the body tries to get rid of the stone.
-
Nausea and vomiting
-
A feeling of an intense need to urinate
-
Abnormal urine color or appearance
-
If fever or chills are present with any of these symptoms, an infection may be present, and you should see your doctor immediately.
Diagnosis
As stones pass out of the body, they irritate the lining of the urinary tract and cause visible blood in the urine in 25 percent of patients and blood that is found on lab analysis (microhematuria) in 95 percent of patients.
Since most stones contain calcium, they can be seen on a plain abdominal X-ray film called a KUB (kidney, ureter, bladder). Stones with a uric acid or cystine composition may be difficult to see on a KUB and many patients will need a sonogram or CT to confirm the diagnosis.
Kidney stone prevention
The first step in starting to do the medical evaluation to prevent more stone events is to have a complete medical history and physical. This will include looking for risk factors for stone recurrence.
Having a family history of kidney stones may increase your risk. A personal history of frequent diarrhea, or inflammatory bowel problems, gout, and urinary tract infection are all risk factors for stone recurrence.
Knowing your eating habits is also helpful because you may be eating foods that are known to raise the risk of stones or may not be drinking enough fluids or eating the foods that protect against stone formation.
Testing for kidney stones
-
Urinalysis
-
Stone analysis (important for first time stone former)
-
Blood studies (evaluate calcium, phosphate, uric acid, electrolytes, creatinine)
-
24-hour urine collection (to evaluate urinary risk factors) on current diet and then repeat if needed on a stone diet to reduce abnormal findings
-
Additional imaging to evaluate for stone recurrence during routine follow-up.
Treatment for kidney stones
Treatment depends on many factors: size, location, composition, urinary tract anatomy, associated symptoms. Options include:
Medical support to help the stone pass
Since most urinary stones are small enough to pass without the need for surgery, with medical support most patients can pass their stone.
Hydration with water and other fluids is important to move the stone down the ureter and out of the urinary tract. If nausea or vomiting are preventing hydration then you need to contact your doctor.
Pain medication may be needed to help control periods of renal colic. If oral pain medication cannot keep pain under control, then further medical attention is needed.
Certain medications have been shown to improve the chance that a stone will pass. The most common medication prescribed for this reason is Flomax (tamsulosin). Tamsulosin has been shown to improve the chance that the stone will pass.
If you develop fever while trying to pass a stone, you need immediate medical evaluation.
Surgery options for kidney stones
Surgery may be necessary if:
-
The stone causes too much pain.
-
Even with time the stone does not pass.
-
The stone is found to be too large to pass spontaneously.
-
The stone is causing severe blockage to the kidney and may cause kidney damage.
-
If the stone is found in conjunction with a urinary tract infection.
Shock wave lithotripsy (SWL)
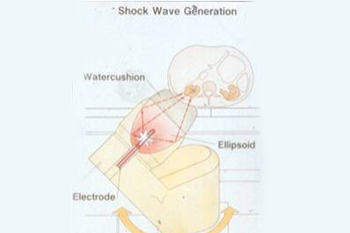
This procedure offers the patient the chance to have the stone fragmented inside the urinary tract without cutting or internal instruments. The technology focuses pressure waves from outside the body to the stone location and with a series of pressure waves delivered over a 1-hour treatment and with the help of general anesthesia, this procedure can break stones small enough to be able to be passed out of the urinary tract spontaneously. Stones in the kidney and ureter can be treated with this technology.
Although many stone patients can be offered SWL, not all stones can be treated with SWL. Stones that are made of cystine and some types of calcium oxalate stones or if larger than half an inch maybe better treated with other technology. Patients may see blood in their urine after the treatment while passing the fragments and some patients may have pain passing fragments.
Ureteroscopy (URL)
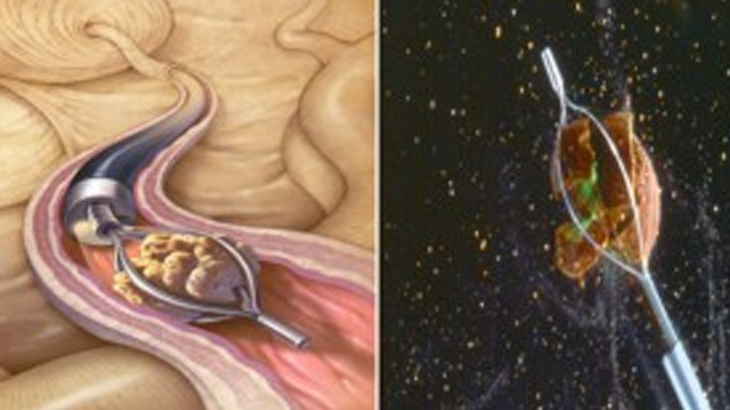
The development of small fiberoptic telescopes both semi-rigid and flexible can now allow your urologist the ability to pass this device into the lower urinary tract through the urethra without an incision. He/she can pass the scope through the bladder and into the ureter and all the way into the kidney if needed, to be able to treat stones in any location.
Small stones can be removed with the use of a tiny wire basket. Larger stones can be fragmented with the use of a holmium laser that creates tiny shock waves that break the stone into small fragments that can be passed out of the ureter. This procedure allows the urologist to visualize the stone during the treatment for safe fragmentation.
Once the stone has been removed or fragmented, the urologist may place a temporary stent in the ureter. A stent is a small soft silicone tube (looks like a piece of green spaghetti) that helps the urine drain from the kidney into the bladder. This stent is completely within the body and does not require an external bag to collect urine.
If a stent is placed, it will need to be removed by the urologist in 3 to 10 days. It is very important that the stent is removed as it can cause complications if left in place for an extended period of time (months).
Percutaneous nephrolithotomy (PNL)
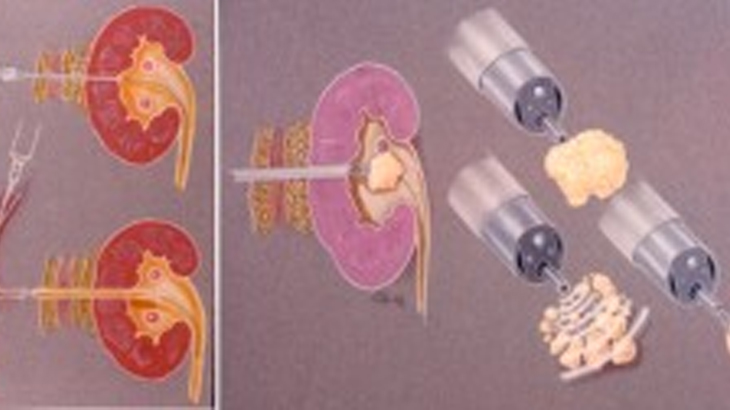
This procedure is recommended when stones in the kidney are too large to treat with SWL or ureteroscopy. PNL involves making a half incision (cut) in the side, after a needle is advanced to the inside of the kidney, a balloon is used to gently dilate an opening large enough for a rigid scope (nephroscope) to be passed from the back into the hollow center part of the kidney where the stone is located.
An instrument passed through the nephroscope breaks up the stone and suctions out the pieces. Grasping forceps can also be used to remove fragments. This ability to fragment and remove fragments from the kidney makes PNL the best option for large stones.
After the stone removal, either an internal stent or external drainage tube is needed to help the kidney recover from the stone removal. Patients usually remain in the hospital at least over night for this operation. Follow-up imaging will determine if all stones have been removed prior to removal of the stent or nephrostomy tube. Patients can usually return to normal activity after about 1-2 weeks.
Laparoscopic/Robotic/Open surgery
These procedures are rarely used to removes stones. They are used only if all other less invasive procedures fail. They require a hospital stay and have a longer recovery period.
All three of the treatment options require anesthesia for the treatment. In most cases general anesthesia is used at our treatment center. This allows safer and more accurate treatment for most patients.
When SWL or PNL is planned, patients are asked to stay off medications that may increase the risk of bleeding for 10 to 14 days. (Aspirin, non-steroidal meds like Motrin, Advil, or Aleve) and some over the counter meds like fish oil, vitamin E, gingko, and St John’s wort.
If patients need to remain on blood thinners for medical reasons, then ureteroscopy and laser lithotripsy may be the best choice. SWL is not an option for pregnant patients.
Our providers
Expert nephrology care
Getting the care you need starts with seeing one of our nephrologists.